
So your client wants to deadlift? That's great, but as you’re aware, deadlifts require an adequate amount of stability and motor control in the hips and lumbar spine. Not everyone can just pick up plates off the floor willy-nilly.
Obviously, the deadlift is a very technical and complex movement to coach. It's crucial to assess if clients could flex their shoulders and whether they have core strength, squat patterning, and single leg balance, to name a few things. Beyond those there is one other thing that many coaches overlook, and it’s so simple:
Can your client touch his toes?
It's a serious question. Your client’s ability to touch his toes is a simple assessment that is commonly associated with hamstring flexibility, and if he can't, it can impede his ability to deadlift and generally move well.
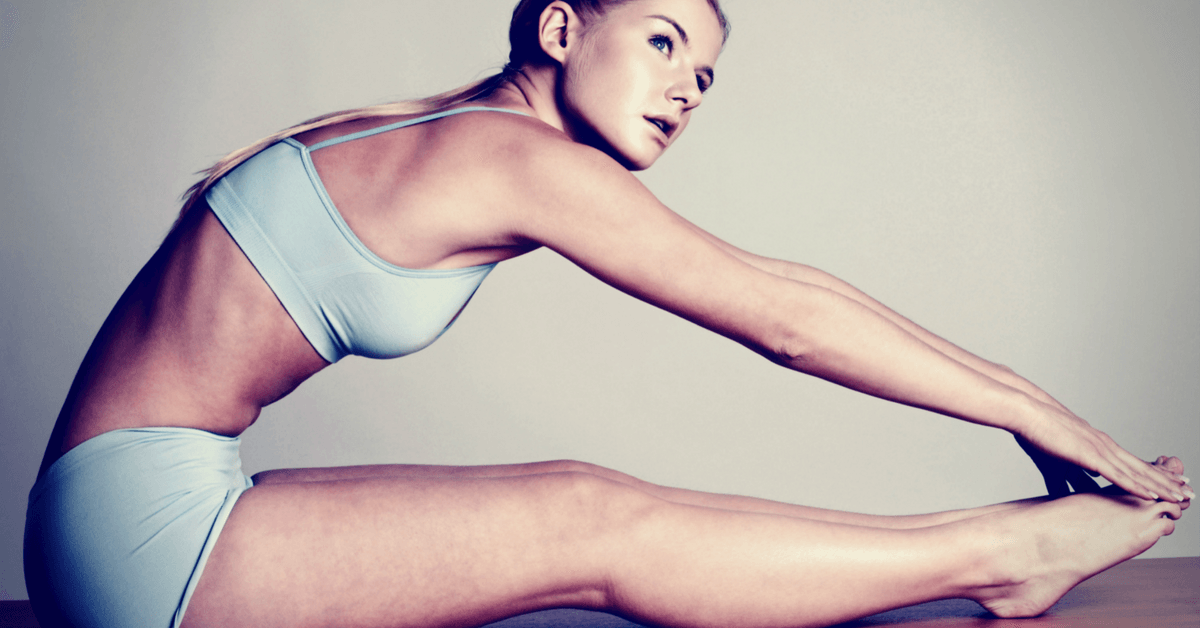
At the same time, something as simple as reaching down to touch your toes is actually a lot more complex than you think. According to the Selective Functional Movement Assessment (SFMA), the toe touch exercise is a multi-segmental flexion pattern which includes the ability to touch the toes without bending at the knees and demonstrate a ‘clean’ movement through the hips and spine.
Basically, it looks like this:

Okay, big deal! Why does this matter to us as trainers whether clients can touch their toes?
Because if they cannot, something is preventing them from touching their toes and loading their hips appropriately. We would need to investigate further to see if the root cause is a mobility or stability problem.
Is it an issue of mobility or stability?
In order to better understand the problem, you must first understand that when a movement dysfunction is present, everything other than the source matters. This is called regional dependence, a concept that was first noted by Gray Cook and Mike Boyle. They observed that the body has a linked relationship between mobile and stable segments, from the feet all the way up to the cervical spine. That means seemingly unrelated impairments in a remote anatomical region may contribute to or be associated with a client who experiences low back pain when bending forward.
Therefore, in order to make the correct assumptions, you must first address the system as a whole, rather than address the problem at its primary location.
A primary example of regional dependence, then, is in your clients who cannot touch their toes.
Here the problem may lie in the limited integrity of the client's lumbar, thoracic, and cervical spine, which prevents the client from flexing the hips in the first place. Or it could be that he just can’t seem to move the trunk and spine with enough coordination to touch his toes. Or maybe his breathing patterns just aren’t optimal.
Clearly, there are many potential causes of dysfunctions. It is natural for abnormal, compensatory patterns to occur in order for the body to get the job done. That said, it is up to you as the trainer to recognize these signs prior to programming.
Here are a few ways that you can start using now.
Exercises to get to the root of the problem
Simply telling your client to reach down and touch his toes can tell you a lot, but it doesn’t get specific enough. I like to have my clients do the following exercises to gain more insight into the root cause. (Remember that if your client has pain at any point, you should refer them to a qualified professional in order to get them properly evaluated.)
Single-leg toe touch
Assuming your clients can’t touch their toes, the next step is to figure out if they have problems on both legs or just one. Have them do the following:
1. Stand with feet together, while barefoot.
2. Shift weight onto one leg, keeping it straight, while bending the other leg and coming up on the ball of the foot.
3. Put their hands on top of each other.
4. Slightly bend forward, aiming for the toes of the straight leg. (Make a note about how far your clients can go and how it feels to them.)
5. Change sides and repeat.
How did your client do? Did he improve on one side versus the other? If you can see a difference in sides, then that could indicate your client has a hip restriction, and you can address restrictions through foam rolling, breathing and hip mobility drills.
Foam rolling
Have your clients grab a roller, and take about five minutes to hit the glutes, calves, hamstrings, and quads.
Supine belly breathing
Breathing is a great way to reduce tone in overactive muscles and reset the system. One of the simplest forms of breathing is on the back. Have your clients lie on their back flat to ground and left leg pulled to their butt to activate the hamstrings. If able, have your clients bring their right arm overhead and place their left hand on their ribs for feedback. Instruct them to take a breath through the nose and drive their breath out and up to fill up the entire diaphragm. On the exhale, have your clients fully exhale and depress the ribs to the ground. Repeat for 5 breaths.
If range of motion stays the same on both sides, then the hips and lumbar spine both may have a problem, and you will want to test the position in a non-weight bearing position to see if their pattern improves. That’s where the next test comes in.
Long sitting test
After doing the single-leg toe touch, this assessment will tell you more of what you need to know. In this assessment, have clients sit down nice and tall with legs straight in front of them, and bend forward to touch their toes.
Did their range of motion improve? How about the pattern? Does it look better?
If they improved, then this indicates that there is an underlying motor control problem.
If nothing has improved, you may have a mobility issue in the hips, lumbar spine, and hamstrings. You can help your clients improve range of motion through soft tissue work on the posterior chain, feet, and mobility drills like the kneeling glute mobilization.
Simple correctives to help address mobility
Soft tissue on foot
One of the most neglected areas of the body is the foot. According to Thomas Myers, author of Anatomy Trains, the superficial line is a myofascial meridian that connects the entire backside of the body and runs from the bottom of the foot all the way up to the eyebrow. The superficial back line also happens to be one reason why your clients hamstrings may feel tight when they bend down to touch their toes. Have your client use a lacrosse ball (or something similar) to roll the bottom of their feet for a few minutes and see if they improve.
Kneeling glute mobilizations
This is a great mobility drill to use for deadlifting because if your client has tight hips they will not be able to hinge correctly.
Have your client start out on all fours in a slightly staggered stance. Place the foot behind the opposite knee on the side you want to mobilize. Once in position, rock the hip back and out on the forward side, and return to starting position.
If they still do not improve after your drills, you can dig further by trying the next few assessments.
Active straight leg raise
With the client lying down on his back, have him perform an active straight leg raise. Per the SFMA, normal range of motion is 70 degrees bilateral. If he is able to attain 70 degrees, then hip flexion is assumed normal.
If he is not able to attain 70 degrees, you should check it passively. Normal range of motion is 80 degrees. If you can get your client to 80 degrees with no problem, it is safe to assume he either has a core or stability motor control problem, or a hip flexion motor control problem.
Then try these correctives.
Core-engaged leg raises with bolster assist
The following exercise will help your client's ability to move at the hips in a low-level position.
To set it up, attach a band to an anchor point that’s located behind your client. Have him lie down on the ground face up, and place a bolster underneath his Achilles. Tell your client to grab the band from behind him and pull it down to his hips to engage his core. Once in this position, raise one leg up and keep one leg on the bolster. Once the leg reaches the client's range of motion, have him forcefully exhale while he returns to the starting position.
Assisted active straight leg raise with band
This one requires a little more core engagement from the client to effectively move through his hips. Anchor a band behind your client and have him attach the band to his foot. While lying down on the ground with both legs straight, have your client press his palms into the ground for core activation and use the band to assist raising the leg. Repeat with both sides.
If your client is not able to raise his leg to about mid-thigh of the opposite leg down, then it could be a hip joint mobility problem and can use the next test to determine where to go.
Supine knees to chest
Make sure your client keeps his knees together and have him pull his knees to his chest while holding his thighs. Normal range of motion is around 120 degrees of hip flexion. If he can flex the hip without the sacrum coming off the ground, it is safe to rule out the hip joint and consider a motor control problem.
However, if he cannot flex the hip, it's safe to assume that there is a hip flexion mobility dysfunction.
And you may have found your culprit behind your client’s inability to touch his toes, which you can try these drills below.
Drills to improve the toe touch
Wall hip flexor mobility
The drill above is a great corrective to address mobility. In a similar fashion, the drill below is my recommendation for addressing motor control.
Quadruped rock-back with core activation
This is a great drill to teach your clients how it feels to move the hips with a neutral spine.
Begin in the quadruped posture by positioning your client on all fours. Your client's feet and knees are little wider than shoulder width apart, feet are plantar flexed, knees in line with his hips and hands in line with his shoulders. Maintain vertical alignment and a neutral spine throughout the exercise. Place a ball against the wall and your client's sacrum on the ball. Tell your client to rock back into the ball and hold the position for a slight pause.
But don’t just assume that the the hips are the problem, as there is one last thing to take a look at before moving on.
Or maybe it's a spine flexion problem?
This is a great test to check unloaded spine flexion. Have your client in a quadruped position and sit back onto his heels and flex his spine as comfortably as he can. You should be able to see a nice uniform curve and full flexion of the spine. If your client presents a nice uniform curve, then you may consider a weight bearing motor control problem of the spine and hip.
If he does not present a nice uniform curve, then there may be a spinal flexion mobility problem preventing the toe touch and you can try this corrective.
Curl-up with pattern assist
This is a great exercise to improve the forward bending pattern. Have your client lie on his back with a miniband around his ankles to create stabilization while grabbing a hold of an anchored band. Proceed to have your client curl up one vertebrae at a time to the desired range of motion.
You are now armed with a number of thorough assessments that can help your clients touch their toes and deadlift better. Remember, do not automatically assume anything, as that could get you into trouble later on in your programming. So check for that toe touch!